In its latest Safety Digest, UK MAIB provides lessons learned from an incident where a coastal bulk carrier passed too close to a quay, resulting in the vessel’s bow making heavy contact with it. The bow was scraped and dented.
The incident
A small, coastal bulk carrier was heading upriver towards its intended berth. It was early morning and there was a moderate breeze on the port quarter and the last of the flood tide; visibility was good but in darkness.
The master, second mate, lookout and a pilot had been on the bridge for the passage upriver. In the approach to the berth the second mate and the lookout went to the forward mooring station, leaving the master and pilot to conduct the berthing manoeuvre. The master’s plan was to swing the vessel to port through 180° and berth starboard side to the quay. As a matter of routine, the master had set a radar range marker 20m offset from the bow as a safety reference to avoid contact with the quay during the turn.
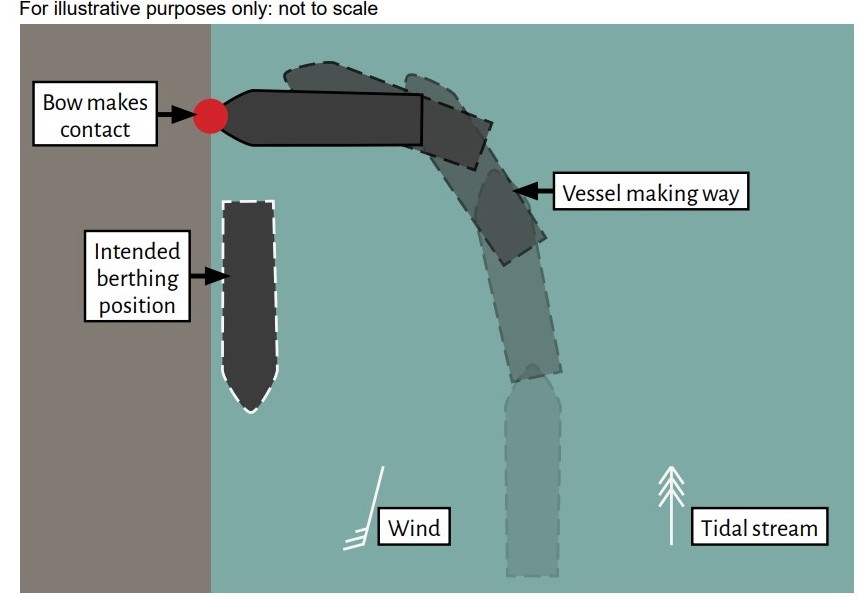
The pilot thought the speed was slightly high just before the turn began, but did not raise concern. The master was controlling the vessel and started the turn using port rudder, slow astern and full bow thruster to port. After swinging almost 90°, the second mate radioed the bridge, warning that the bow was passing too close to the quay; however, this came too late for the master to take effective avoiding action and the vessel’s bow made heavy contact. The bow was scraped and dented and the impact left a paint mark on the quay wall, although it was undamaged.

Lessons learned
#1 Plan: Passage plans are ‘berth-to-berth’ for a reason: to ensure that there is a careful plan for every phase and that it is properly executed. In this case, neither the wind and tidal stream effects nor the optimum speeds were considered in the berthing plan. A safer course of action might have been to reduce speed earlier and then use the wind and tidal stream to aid a turn at rest, with little or no headway.
#2 Communicate: Pre-arrival briefings that incorporate the pilot are significant milestones in delivering a shared mental model. Such briefings should include the forecasted and actual weather conditions, planned speeds, and expected safe passing distances of navigational hazards. Only then can navigational decisions or deviations from the plan be challenged. The master should encourage all crew and the pilot to speak up where there is uncertainly; such challenge should then be acted upon or the reason given for why it is not.
#3 Action: The forward mooring station did not provide regular updates on the distance to the quay. A single report was made, which came too late to take avoiding action. To avoid misunderstanding, early and regular reports on closest points of approach and actual distances should be clearly communicated.
#4 Monitor: Use of a radar range marker was a reasonable safety barrier to aid the turn; however, it needed to be monitored. The master directed his attention to handling the vessel and other crew members, who could have assisted him, had left the bridge and gone to their mooring stations. Good bridge team management can help to alleviate these situations by making sure everyone knows their role and that navigation aids are effectively monitored for signs of danger.