













Transport Malta’s Marine Safety Investigation Unit (MSIU) issued an investigation report on the fatality of a crew member onboard the Maltese-registered chemical tanker ‘Scot Berlin’ in August 2017. According to the report, the ‘immediate cause of the accident was the entry into a space which had a significant presence of toxic gases suspended in the air’.
Namely, the investigation report cites that the cause of death was identified as cardio respiratory failure. However, at the time of writing the safety investigation report, the autopsy and toxicological reports had not yet been released by the local authorities.
Input from the legal representatives of the owners suggested that ”currently, the investigation is still ongoing along with the Incident Report and Autopsy report which are in the course of preparation”.
Excerpts from the final safety investigation report follow, which published within August by Tranport Malta, summarizing the course of events that led to the fatality and citing related safety issues and other findings.
The incident
The vessel arrived at Marsaxlokk Oil Tanking Terminal loaded with two parcels of cargo. Following the completion of cargo operation, the crew members started the ballasting of the vessel since her next trip to Spain was a ballast voyage. Ballasting in the forepeak tank started under the supervision of the second mate.
About an hour later, at about 1300, a high bilge level alarm in the bow thruster compartment sounded on the vessel’s Alarm Monitoring System. The bosun proceeded forward to investigate. He immediately noticed water escaping from the forepeak tank’s manhole, reaching the bow thruster entrance, flowing over the sill plate and cascading on the bow thruster motor.
Consequently, one of the bilge alarms in the bow thruster compartment triggered the high level alarm. Aware of possible issues with the bow thruster motor, the chief engineer instructed the electrician to inspect the motor for any water damages. Prior to the commencement of the work, three safety documents were signed. The bow thruster electrical supply to the ventilation fan and the bow thruster motor was isolated.
As part of the cleaning process, the electrician sprayed the motor with an electrical cleaner using a pneumatic spray gun. He then proceeded to the messroom and returned to the bow thruster compartment at around 1600. About 20 minutes later, the bosun went to check on the electrician and found him unconscious, lying over the bow thruster tunnel.
Crew members were mustered and attempts made to lift the electrician from the bow thruster compartment. Eventually, shore assistance was requested and personnel from the local Civil Protection Department lifted the electrician to the open space on the forecastle deck. However, he was pronounced dead onboard.
Key Findings
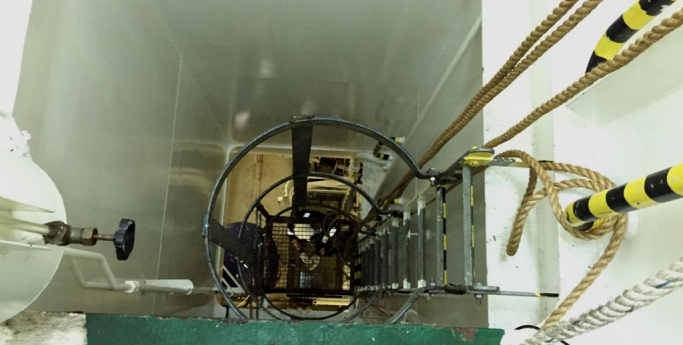
One of the interesting comments of the investigation are related with the conditions inside the bow thruster compartment.
According to the report, The fact that the occurrence happened inside the bow thruster compartment necessitated an analysis of the internal environment, i.e., the bow thruster space. IMO Resolution A.1050(27), adopted on 30 November 2011, provides a set of revised recommendations for entering enclosed spaces on board ships. All preventive and protective barrier systems relevant to enclosed spaces depend on whether the space is actually considered as enclosed.
The IMO Assembly Resolution defines an enclosed space as one with the following characteristics:
1. limited openings for entry and exit;
2. inadequate ventilation; and
3. is not designed for continuous worker occupancy
The Resolution then goes on to present a list of spaces which are considered as
enclosed spaces. Bow thruster compartments are not included in the list, although the document makes it clear that the list is not exhaustive.
Transport Malta’s MSIU notes that the ISM Manager of the vessel did not consider the bow thruster as an enclosed space and consequently, this space was not addressed as such in the SMS.
The safety investigation was also of the view that the bow thruster compartment did not classify as an enclosed space on the basis of:
- the opening, which was not limited and was adequate and provided a safe
means of access; - the ventilation, which was mechanical and provided adequate flow of fresh air from the outside on the main deck; and
- the space was adequately lit artificially through the access shaft, down to the actual bow thruster space.
By virtue of the above, the preventive (corporeal) barrier systems focused on the hazard related to the bow thruster motor, i.e., electric shock. The MSIU believes that the environment inside the bow thruster compartment had changed to a hazardous one just before the accident happened for two main factors:
1. presence of toxic, flammable, vapours; and
2. absence of proper ventilation.
As a direct result of the change in the bow thruster compartment conditions, the safety investigation concluded that at the time of the accident, the bow thruster compartment’s characteristics were similar to those of an enclosed space, without actually being declared as such. – Transport Malta MSIU comments
Important Notice: Transport Malta outlines several issues from the investigation, highlighting that ”the following conclusions and safety actions shall in no case create a presumption of Blame or liability; neither are they listed in any order of priority”
Safety issues
- Preventive (corporeal) barrier systems focused on the hazard related to the bow thruster motor, i.e., electric shock;
- The environment inside the bow thruster compartment changed to a hazardous one just before the accident happened;
- At the time of the accident, the bow thruster compartment’s characteristics were similar to those of an enclosed space without being declared as such;
- The hazard and precautionary statements related to the use of the chemical were not discussed on the day of the accident;
- The electrician was not wearing any respiratory safety equipment;
- The limited amount of volume of chemical used may have led the electrician to believe that the extensive protective clothing was not required in this case;
- The isolation of the auxiliary switchboard resulted in the switching off of the bow thruster compartment ventilation, compromising the supply of fresh air inside the space;
- Vaporised cleaning chemical would have been entrapped inside the bow thruster compartment;
- It was not excluded that the electrician may have also lost his grip and fell from the lower section of the ladder / lower platform onto the bow thruster tunnel while holding the bottles of fresh water;
- The use of the electro cleaner (and the way it was applied) was critical, safety information that had not been communicated;
- The risk involved with the carriage of the three water bottles while going down the ladder was considered manageable by the electrician and it would have necessitated neither the assistance of other crew members nor the need to lower the bottles by a rope before going down the ladder;
- The electrician was unable to make use of knowledge and skills which his colleagues could have contributed towards a safer task.
Other findings
- At the shipyard, the physical and mental demands were high and the vessel’s schedule would have barely left time to the crew members to recover, not to mention the inevitable interruptions and other distractions which one would expect to encounter in similar places;
- Under high workload conditions, attention to all specifics in detail is simply difficult to achieve;
- Such is the nature of work at a shipyard that it is very likely that a necessary check (e.g. that all manhole covers are tight) is omitted because of some local distraction;
- Considering the nature of the work in the dry-docks, it was not excluded that the details in the documentation, time pressure, and coordination and communication breakdowns may have contributed to the omission of checking the tightness of the manhole cover;
- The bow thruster compartment did not classify as an enclosed space;
- The electrician was most probably going down the ladder but also somewhere close to the ladder’s lower platform;
- The chief engineer neither saw the electrician carrying the electro cleaner nor was he aware that the electro cleaner was actually used to clean the motor;
- The use and application of the electro cleaner was an initiative, which was adopted with all good intentions to minimise as much as possible the damage to the electrical components of the bow thruster motor;
- The nature of the tasks and the competence of the electrician were perceived as not necessitating formal team / group collaboration;
- At a time when team dynamics should have been applied, the complexity and urgency of the circumstances contributed to a condition where the master took initiatives of his own and even accessed the bow thruster compartment where, on his way down, he could smell a strong, chemical odour;
- The master accessed the bow thruster compartment without a rescue harness and safety lines, possibly because these may have been viewed as a hindrance to act quickly and time consuming to don at such critical time;
- The emotional preferences chosen by the master, who opted to make the (personal) entry initiative were seen to be more efficient in achieving the intended goal of (possibly) saving a crew member inside the bow thruster compartment;
- Rather than having a faulty perception of potential losses, the master had a positive affect associated with the perception of potential opportunities, i.e. saving the life of the electrician.
Actions taken
Safety Actions Taken During the Course of the Safety Investigation
- During the course of the safety investigation, the ISM Managers took the following safety actions, intended to prevent a recurrence of a similar accident:
- An internal safety investigation report, compiled in accordance with Section 9 of the ISM Code, has been circulated on all Company managed vessels for training purposes
- An entry procedure for non-enclosed spaces with a vertical ladder has been
drafted and implemented on board. The procedure includes STOP cards,
notification posters and recovery procedures; - The procedures addressing the handling of chemicals and their restricted use has been strengthened and is now part of the work permit process
- The dry-docking procedure has been revised. A new section in the Company’s ‘Dry Docking Safety Checks’ Form has been introduced to ensure a thorough check of all areas prior to refloating;
- Drills for ‘rescue from enclosed spaces’ have been amended and are now more detailed. The frequency of the drills has also been increased.
Finally, in view of the conclusions reached and taking into consideration the safety actions taken during the course of the safety investigation, MSIU notes that no safety recommendations have been made.
Find out more herebelow: