






























BSU published its investigation report on Seoul Express, when on 27 March 2021 a crew member fell from a vertical cargo hold ladder in cargo hold no. 3 and lost his life.
The incident
On 27 March 2021, the SEOUL EXPRESS was approximately 52 nm off the coast of Mexico en route from Manzanillo in Mexico to Long Beach in the United States. The ship was engaged in regular service between various ports in the Mediterranean, Central America and the west coast of North America.
At the end of his morning watch, the later deceased first watchman of the 4-8 watch (deployed at sea as a lookout, referred to below as ‘watchman’) began the usual inspection of the temperatures of the loaded fish meal containers at 0700 on the instructions of the chief mate, who was in charge of the navigational watch. This involved checking 11 containers in Bays9 10, 29 and 31 during the voyage in question. Daily temperature inspections of fish meal are required because this cargo is assigned (depending on composition) to the dangerous goods classes 4.2 and 9 according to the IMDG Code10, which means it is a spontaneously flammable substance. A contactless laser or infrared thermometer can be used for this.
During his inspection, the watchman used a UHF13 handheld radio to send regular reports to the officer on watch on the bridge – always upon entering and leaving each cargo hold (CH) in accordance with standard operating procedures.
At 0715, the watchman reported the entry and then shortly afterwards exit from CH1 for the inspection of the containers in Bay 10. At 0730, the chief mate was notified that the watchman was reportedly now entering CH3 in Bay 29. The four fish meal containers stowed in Bay 29 were below deck in the lowest tiers (02, 04, 06 and 08) and in Row 01 situated in the middle slightly to starboard.
Since no further report on leaving CH3 was received on the bridge and the watchman could not be contacted by radio, the chief mate informed the master before it had turned 0800. A search for the overdue crew member was then immediately initiated. The chief mate formed a search party consisting of himself, the bosun, two ABs and one unskilled deckhand (OS). At the same time, the chief mate instructed the 2nd engineer and two cadets to check the watchman’s cabin.

At 0809, the search party found the access hatch to CH3 in Bay 29 open. The chief mate used a gas detector to test the atmosphere in the cargo hold and identified neither low oxygen levels nor dangerous gases. He then entered the cargo hold, climbed down to the next lower deck using the ladder beneath the access hatch and called out for the watchman. He received no answer and climbed down to the next deck. He was then able to see the missing person lying motionless on the 4th stringer deck. The chief mate decided to carry out the subsequent evacuation with respiratory protection.
At 0817, the chief mate and an AB entered CH3 wearing respiratory protection and reached the casualty on the 4th stringer deck two minutes later. The latter was lying chest down with his head face down and turned slightly to the left, his arms resting against his torso and his legs outstretched. He had a bleeding wound on the back of his head and was unresponsive. The chief mate tried in vain to find a pulse on both the neck and wrist.
The unconscious casualty was secured at the scene with a rescue sling at 0826 and evacuated to the hatch cover (top deck), where he was placed on a spineboard16, at 0834. A rope and snatch block system suspended between containers on the top deck was used for the evacuation. A more detailed examination and first aid were carried out on the top deck but the casualty continued to display no vital signs. Cardiopulmonary resuscitation was started directly in the transverse corridor next to the access hatch at 0838 and an AED was used to resuscitate the watchman. Since there was no ventricular fibrillation and no discernible heartbeat, the AED did not deliver a shock. The casualty displayed no vital signs.
Analysis
#1 Risk of Falling: In the present case, no sufficient measures were taken to adequately minimise the probability of occurrence and/or the severity of impact of a fall when using long cargo hold ladders. Although access to the cargo hold ladder is clearly visible due to the coloured access hatch with labelling on the inside of the cover, i.e. people cannot accidentally step into the companionway and are not exposed to any sudden danger, the BSU believes there is still a risk of falling from the actual ladder. Causes may include slipping because of dirt and/or moisture, ill-fitting protective clothing, fatigue, carelessness or a loss of balance due to a wide range of different factors. The severity of the impact of a fall is increased by the falling height due to the length of the ladder(s) and poor accessibility of the lower decks with the rescue stretcher.
On board the SEOUL EXPRESS and on comparable container ships, the need to use long vertical ladders in cargo holds several times a day also increases the probability of a fall, at least whenever refrigerated and/or dangerous goods containers have to be checked in the hold on a daily basis. Accordingly, the BSU believes that the use of PPEaF is appropriate for falling heights of more than 2-3 m. In particular, measures should be taken to ensure that the user is not hindered unnecessarily while descending/ascending when such ladders have to be used frequently. Accordingly, an energy absorber with two safety hooks is not considered practicable in this particular case. Firstly, its correct use would significantly increase the time required for such daily routine activities, and secondly, the ladder is gripped with only one hand during the continuous repositioning of the safety hooks.
#2 Atmosphere Hostile to Life: Due to the permanent mechanical ventilation of the cargo hold, the result of the atmospheric measurement by the chief mate shortly after the accident and the autopsy report, the BSU does not believe that the accident was caused by a lack of oxygen or toxic gases. However, since ordinary gas detectors cannot identify all dangerous gases, gas poisoning cannot be ruled out with absolute certainty and wearing respiratory protection while rescuing the casualty was therefore justified.
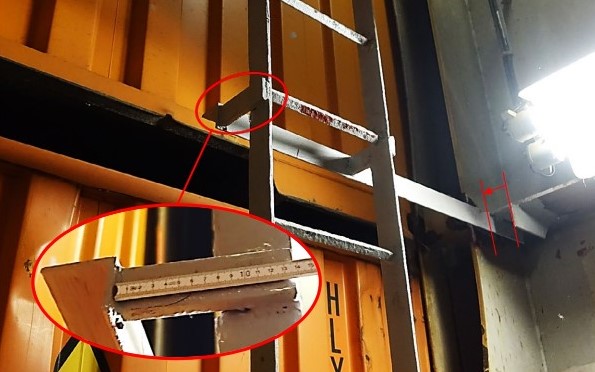
#3 Risk of Falling in the Cargo Hold: The dimensioning of the access hatch, the deck passageways and the hold ladders in CH3 on the SEOUL EXPRESS comply with applicable regulations for container ships of this size and year of construction. However, due to the lack of horizontal clearance (less than the required 15 cm) between the hold ladder and fixed components (support strut as well as load-bearing upper plating and horizontal section of the bulkhead) between the 2nd and 4th stringer deck, the requirements of Section 21(5) DGUV Regulation 84 are not met.
The ladder’s welded lateral support struts give rise to a slanted step on one of the rungs, especially between the 2nd and 4th stringer decks, and also make them harder to grip. This can impair safe access to the cargo hold. It has not been possible to conclusively determine the extent to which this contributed to or was a factor in the accident.
Probable cause
The specific cause of the watchman’s fall could not be determined. However, several factors were identified that may have contributed to or facilitated the occupational accident. Some of these have also been identified in similar accidents in the past.
Under the management of the ship operator of the SEOUL EXPRESS, another fatal accident already occurred in 2019 due to a fall from a greater height in a cargo hold (see BSU Investigation Report 452/19 SAJIR). The generally high number of fatal accidents involving falls on container, bulk and general cargo ships with similar facilitating circumstances suggests that risk minimisation (taking into account the hierarchy of measures) is necessary to reduce the number of accidents.
The IMO has already identified a corresponding need for action and a working group was commissioned with the analysis of accident investigation reports on falls from greater heights and the deduction of appropriate recommendations. It was identified that tasks involving the risk of falling, are not always considered as hazardous work, so that no appropriate measures for preventing falls or minimising their impact are taken.
EXPLORE MORE AT bsu’S accident REPORT




























