














The Nautical Institute presents an incident where, a passenger vessel berthed and the crew was preparing to move the gangway from deck 2 to deck 1 to accommodate the tidal range, which was lower than at the last port.
Extra deck crew were asked to assist with the move, although they were unfamiliar with this task. A work supervisor was responsible for the procedure and for overall safety. This person had several other areas of responsibility. Many tasks were lined up for the deck crew that day, and there was a sense of time pressure.
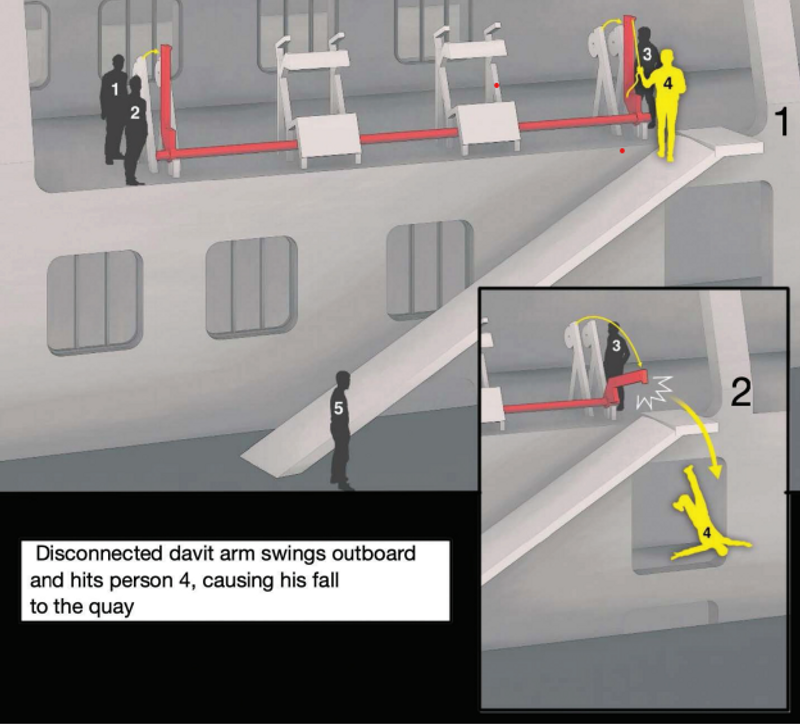
The crew first dismantled the railing and the gangway safety net so that wire rope cables could be connected. The crew involved in the work still had to use the gangway to get up and down from the quay area, despite the dismantling of the safety features. On deck 2, three people were initially involved in the work on the gangway. Person 3, operating the winch, had not done so before and was given an introduction to which buttons to press by person 4, who had more experience with the winch and gangway. Person 1 observed the work from the forward part of the davit and Person 2 watched the cable of the forward davit.
The davit was hoisted back into its cradle so that it would not obstruct access to the gangway. The davit stuck in the vertical position, and when the cable was run out further, it became slack, while the davit remained vertical. Person 4 moved from the deck onto the gangway and pulled the cable in an attempt to loosen the davit. Person 3 was told to stop the winch and put the control down. With the cable now slack, there was nothing to prevent the davit from pivoting back down to the horizontal position. As it pivoted down it struck person 4, who lost his balance and fell to the quay. First aid was administered and he was taken to a shore hospital by helicopter. He was later pronounced deceased as a result of the injuries sustained in the fall.
The investigation found, among other things, that the crew did not consider gangway rigging tasks to be ‘work at height’. The crew had experience rigging the gangway from deck 1, which was lower, but not from deck 2.
The accident sequence revealed that the work method needed from deck 2 was different compared with that from deck 1; from deck 2 the davit had to be brought back to the cradle so as not to obstruct free passage of the gangway.
The crew did not habitually wear helmets or fall protection equipment for this job when it was performed from deck 1, nor did they do so when working from on deck 2 on the day of the accident.
Lessons learned
-
A ‘dynamic risk assessment’ process is a technique whereby workers constantly scan the workspace for hazards and make the necessary adjustments. In this case, the method of work for gangway manipulation from deck 1 was used, although the work was being carried out on deck 2. A dynamic risk assessment process should have identified that deck 2 presented a new hazard – work from height.
-
Working from height requires fall protection. Working on deck requires hard hat protection regardless of the task or location.
-
Time pressures are usually self-imposed. Even if time pressures are overtly expressed, the proper mindset should be ‘Safety First’.