






























The German Federal Bureau of Maritime Casualty Investigation published its report about an accident with subsequent loss of life on board, concerning the Containership SEOUL EXPRESS, on 27 March 2021.
The incident
On 27 March 2021, the container ship SEOUL EXPRESS was about 52 nm off the Mexican coast en route from Manzanillo, Mexico, to Long Beach, USA. The vessel was operating on a liner service between various ports in the Mediterranean, Central America and the west coast of North America.
Towards the end of the morning 4-8 watch, the watchman began his usual round of checking the temperatures of the loaded fish meal containers at 0700 on instruction of the Chief Officer. For this purpose, eleven containers in the bays 10, 29 and 31 were to be checked on this voyage. Since fish meal, depending on its composition, is assigned to the dangerous goods (sub-) classes 4.2 and 9 in accordance with the IMDG Code and thus to substances liable to spontaneous combustion, daily temperature checks of this cargo are necessary, e. g. by means of a contactless laser thermometer.
Using VHF (very high frequency) hand-held radio, the watchman regularly reported from his rounds to the officer on watch on the bridge – according to standard procedure, always when entering and leaving each individual hold.
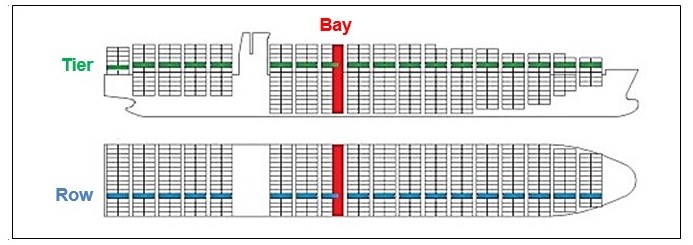
At about 0715, the watchman reported entering and shortly afterwards leaving the cargo hold No. 1 to inspect the containers in bay 10. At about 0730, the Chief Officer received a message from his watchman over handheld radio that he was now entering the cargo hold No. 3 in bay 29. The four fishmeal containers stowed in bay 29 were below deck in the lowest tiers (02, 04, 06 and 08) and in row 01, located midships, slightly to starboard.
As there was no further report of the watchman leaving hold No. 3 received on the bridge and the watchman could not be reached by radio the Chief Officer notified the Master before 0800. A search for the missing crewmember was then immediately initiated.
Since the accident occurred shortly before all crewmembers in the dayshift started work, many helpers could be mobilized for the search without sounding the general alarm. The Chief Officer formed a search party consisting of himself as well as the Bosun, two able seafarers (ABs) and one ordinary seafarer (OS). At the same time, the Chief Officer instructed the Second Engineer and two cadets to check the cabin of the missing person.
At about 0809, the search party found the access hatch to cargo hold No. 3 in bay 29 open. The Chief Officer checked the atmosphere in the cargo hold using a gas detector and determined neither a low oxygen level nor hazardous gases. Thereupon, he entered the cargo hold, descended the ladder below the access hatch by one deck and called out for the watchman. He did not receive an answer and descended one deck further. From there, he could see the missing person lying motionless on the No. 4 stringer deck. The Chief Officer decided to carry out the further evacuation using a self-contained breathing apparatus (SCBA).
Meanwhile, after the Chief Officer’s report, the Master first went to the ship’s office to speak with the Chief Engineer. During the conversation, the Second Engineer entered the ship’s office and reported an injured person and that a rescue stretcher would be required. Since the Master had a key for the ship’s hospital with him, which is located on the same deck as the ship’s office, the Master and the Second Engineer went to the ship’s hospital without further ado.
There, a spineboard and a craneable rescue stretcher with integrated vacuum mattress were available. According to his own statements, the Master decided in favour of the narrower and more manageable spineboard because at that point he had assumed that the injured person would have to be evacuated via the access hatch and the vertical ladders. In addition, he did not yet have any information about how seriously injured the person to be recovered was.
While the engineers brought the spineboard to the scene of the accident, the Master went to the bridge and first obtained information about the ship’s position and speed, distance from land (about 52 nm) and traffic volume (very calm, little traffic).
Then, he instructed the Second Officer on watch to gather some information, inter alia, regarding the responsible MRCC. According to his own statements, the Master still assumed at this point that the injured person might have to be recovered by helicopter. For further assistance, he also ordered the navigating officer, who was not on watch at that time, to be called to the bridge, which is what happened thereafter. In addition, the Master prepared the satellite telephone, checked the reception, switched on his handheld radio and took over the internal communication.
At about 0817, the Chief Officer and an AB (AB1) descended into the cargo hold No. 3 both wearing a SCBA and reached the casualty two minutes later on the No. 4 stringer deck. He suffered a bleeding wound at the back of his head and showed no reaction. The Chief Officer tried in vain to find a pulse on both the neck and wrist. He informed the Chief Engineer at the access hatch that the injured person should be pulled up by means of a rescue sling.
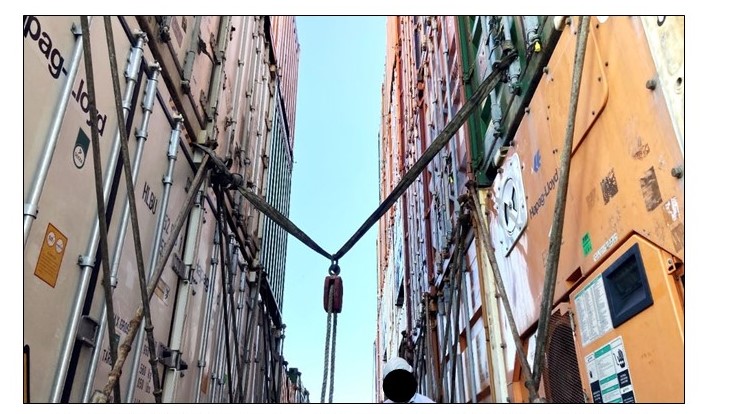
The Chief Officer ascended the ladder again in order to prepare the rescue rope, which had to be attached to the loaded containers or their lashing materials due to the lack of suitable fastening points (see Figure 4). Meanwhile, another AB joined them, equipped himself with a SCBA, descended to the No. 4 stringer deck together with the Chief Officer and AB1, and helped to first lift the unconscious watchman into the sling and then to lead him upwards by the rope. The Chief Engineer and Bosun operated the rope at the access hatch.
The designation of the individual decks of the SEOUL EXPRESS as well as the descent into the cargo hold via the staggered ladders can be understood:
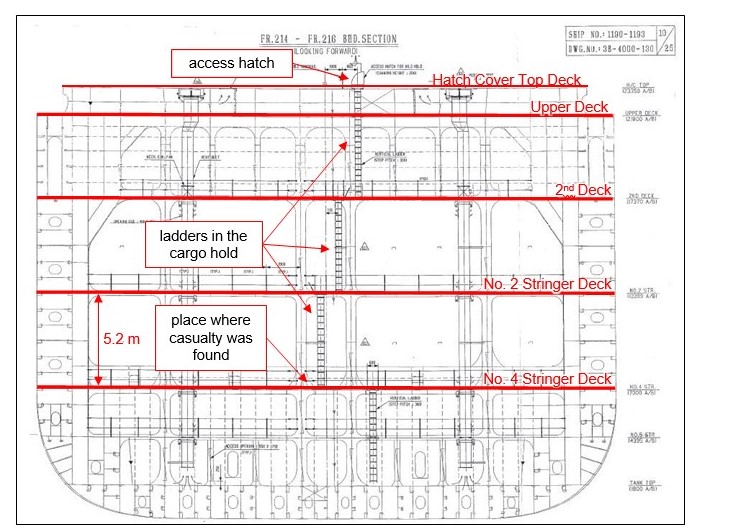
Next figure shows the view from the No. 2 stringer deck to the No. 4 stringer deck below, where the injured watchman was found at the base of the vertical ladder, his helmet and gloves also visible in the picture.

At about 0826, the unconscious was secured on scene by a rescue sling and about eight minutes later evacuated on the hatch cover top deck, where he was placed on a spineboard.
A detailed examination was carried out and first aid administered with the result that the accident victim still showed no vital signs. At about 0838, cardiopulmonary resuscitation was started directly at the scene in the transverse corridor adjacent to the access hatch, also using an automated external defibrillator (AED), in order to revive the watchman. Since there was no ventricular fibrillation and no heartbeat was detected, the AED did not deliver a shock. The casualty had no vital signs.
When the Chief Officer requested medical assistance via radio, the Master immediately went to the scene of the accident. When he arrived, the casualty had already been evacuated to the transverse corridor between bays 27 and 29, where resuscitation measures were carried out.
At about 0900, the unconscious watchman was taken to the ship’s hospital by spineboard on the Master’s instructions. There, resuscitation was continued and another unsuccessful attempt was made to revive the watchman using the defibrillator (no shock was delivered by the AED).
At about 0955, the ship’s command notified the Designated Person Ashore (DPA) of the shipping company Hapag-Lloyd of the accident.
At 1010, the resuscitation measures were without success and consequently discontinued.
In the evening of the following day, the SEOUL EXPRESS reached Long Beach anchorage (Outer Harbour Anchorage) and anchored there at 1948 local time (UTC – 7).
At 2200 local time, three forensic scientists from the Long Beach City Coroner Team embarked the ship to examine the deceased and transported him ashore an hour later.
Analysis
On 29 March 2021, the shipping company Hapag-Lloyd notified the Federal Bureau of Maritime Casualty Investigation (BSU) of the occupational accident resulting in a fatality on board the SEOUL EXPRESS off the Mexican coast. The ship is operated in the so-called “Mediterranean Pacific Service” and sails regularly between Vancouver, Canada and Livorno, Italy. A round trip takes approximately three and a half months and the ship usually calls at 13 different ports in nine countries.
Due to the worldwide COVID-19-pandemic and the associated travel restrictions, the BSU was unable to inspect the ship timely and conduct personal interviews with the crewmembers.
The scene of the accident on board and further circumstances relevant to the investigation were inspected by the BSU in the port of Valencia on 19 October 2021. However, at that time, no crewmembers who were members of the crew on the day of the accident were on board.
Voyage Data Recorder (VDR) data from the time of the accident was not saved on board, so that neither recorded ship data nor audio recordings from the bridge are available for evaluation. Therefore, the investigation is based on:
- written information provided by the ship’s operator:
#1 accident notification,
#2 Master’s statement of facts,
#3 excerpts of the bridge logbook,
#4 internal procedural instructions and documents,
#5 investigation report of the law firm “Gordon&Rees Scully Mansukhani” investigating on behalf of the ship operator’s P&I Club on site in Long Beach,
#6 e-mail conversation with respect to the in-house accident investigation,
- the result of several personal conversations between the BSU and the ship operator as well as the Master and Chief Officer of the SEOUL EXPRESS on 11 and 23 August as well as a video conference on 27 January 2022,
- findings gained from the inspection on board by the BSU on 19 October 2021,
- AIS data from the ship at the time of the accident extracted from the European SafeSeaNet Ecosystem,
- discussions between the BSU and the BG Verkehr(Prevention Division as well as Ship Safety Division, Maritime Medical Service) as well as
- a conversation between the BSU and the classification society
As the watchman involved in the accident had started his daily round to check the temperature of the dangerous goods containers alone and unaccompanied, there were no witnesses who observed the accident directly. Furthermore, there are no image recordings or the like since the accident site on board was under camera surveillance.
Factors that contributed to the accident
In the course of the preliminary accident investigation (primarily evaluation of the files) several factors were identified that could have contributed to the accident and its consequences. These were then investigated more closely.
They include inter alia:
- general dangers when working at height,
- implementation of the occupational health and safety on board,
- the general ship design framework (ladders in cargo holds with the risk of falling),
- the health condition and the fitness for sea service of the casualty,
- the emergency response management of the crew and
- the safety culture on board and in the company as well as the implementation of ISM Code.





























